Suspect XLH?
Connect their symptoms and accurately diagnose with the right tests.
These issues can impact the social and emotional wellness of children and adults.1,3 Getting an accurate diagnosis and early disease management can help minimize the burden of XLH.
Hypophosphatemia, a characteristic of XLH, typically manifests as rickets and osteomalacia in children.3
These lower extremity abnormalities create a significant burden on their daily lives.3
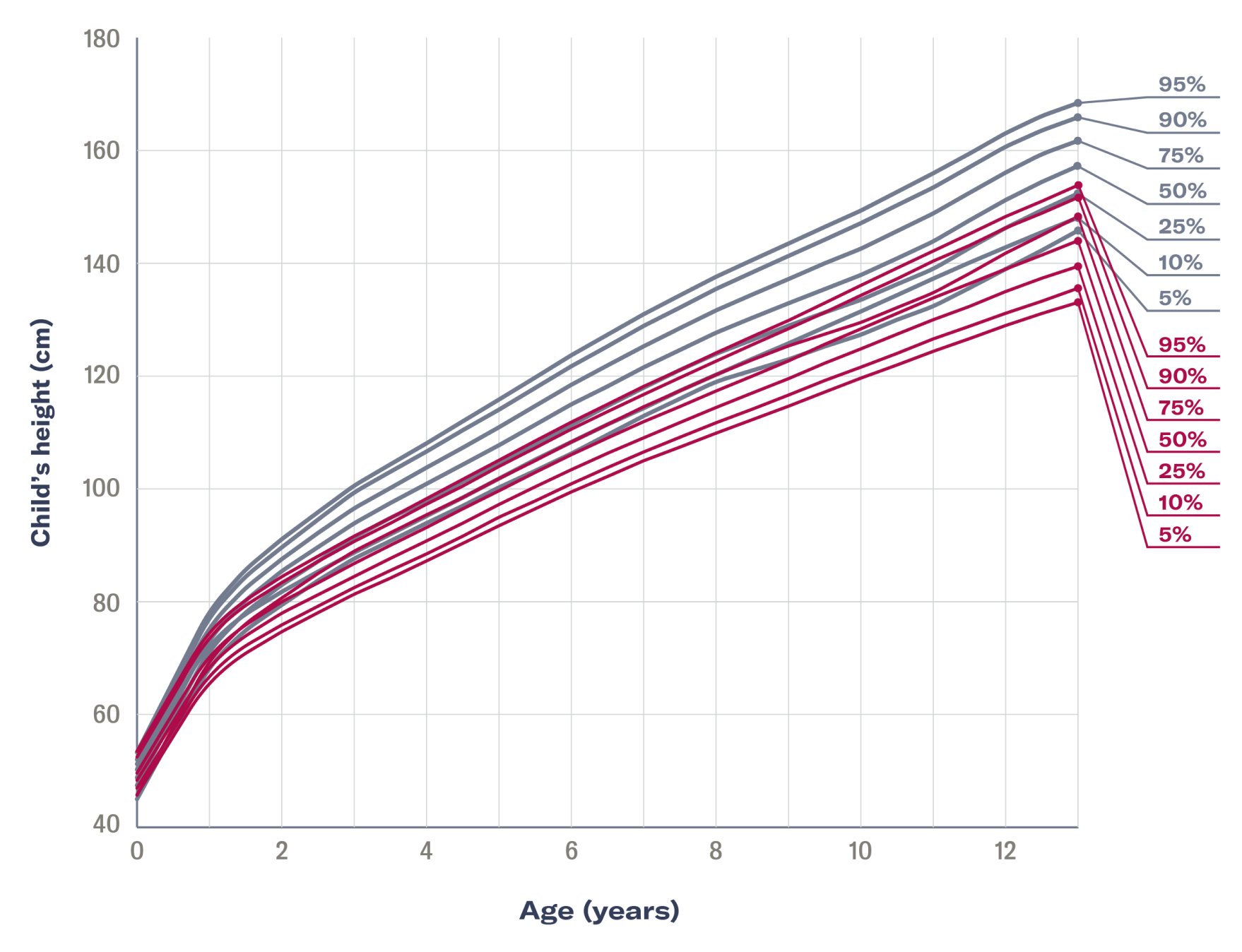
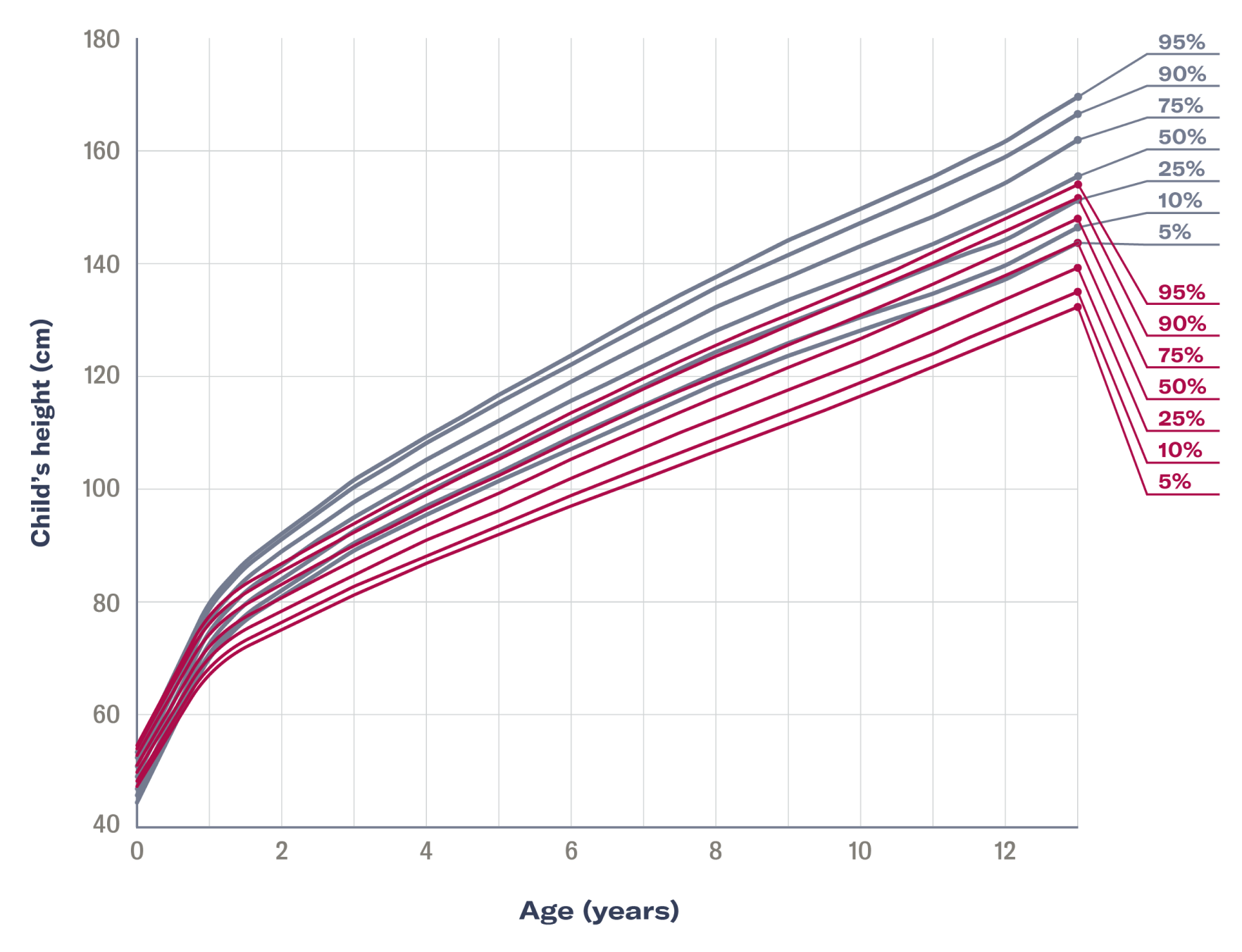
The annual height increase in children with XLH begins to deviate from that of healthy children at 6 months of age and progressively declines during early childhood.4


A 2019 survey* showed that children with XLH scored well below the US general population average for basic mobility, physical functioning, pain/comfort, and happiness.3

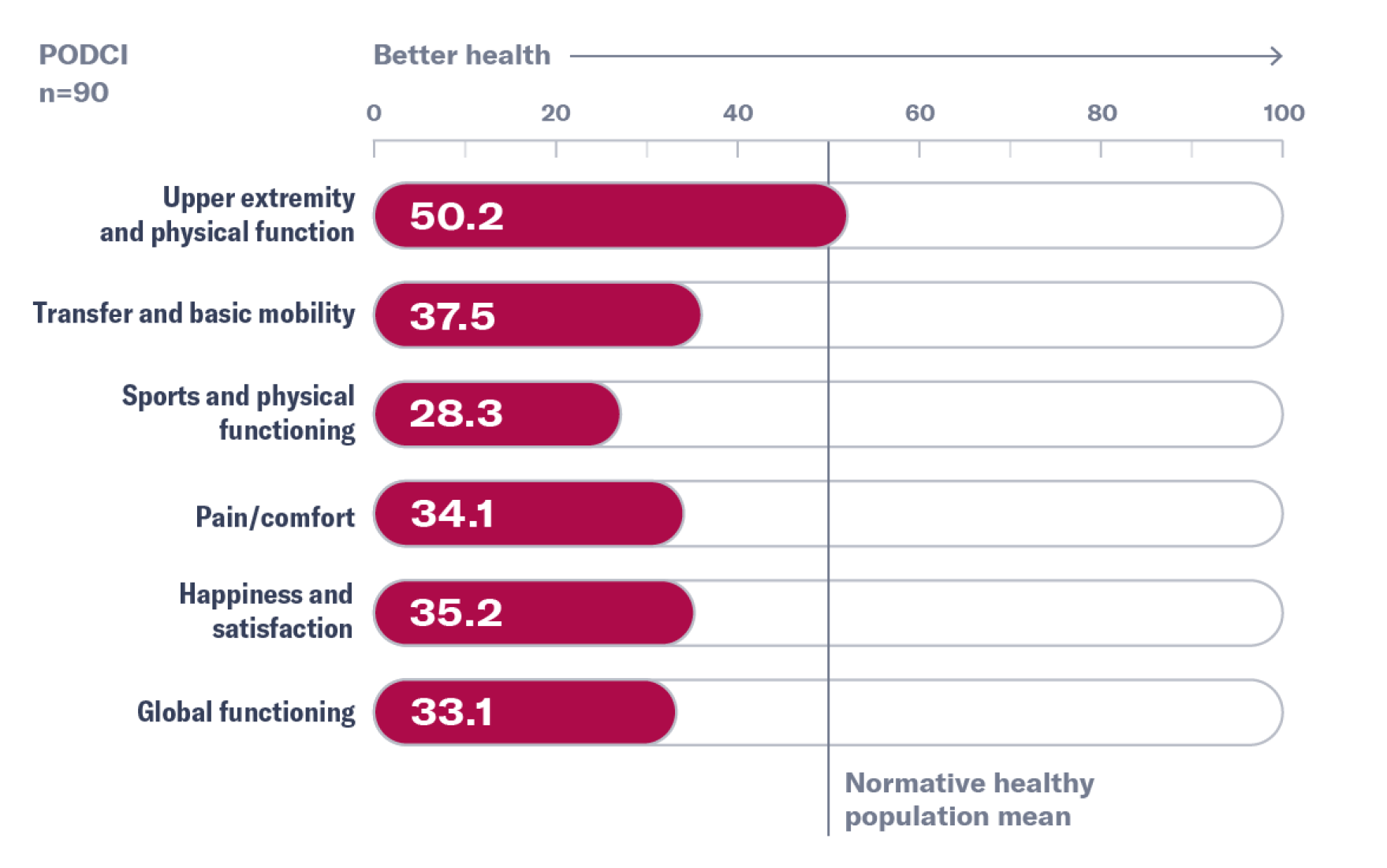
The Pediatric Orthopedic Society of North America Pediatric Outcomes Data Collection Instrument (POSNA-PODCI) score is a parent-reported questionnaire to assess overall health, pain, and ability to participate in normal daily activities, as well as in more vigorous activities associated with children. It contains 7 scales that include upper extremity and physical function, transfer and basic mobility, sports/physical functioning, pain/comfort, happiness, satisfaction, and expectations.3,6
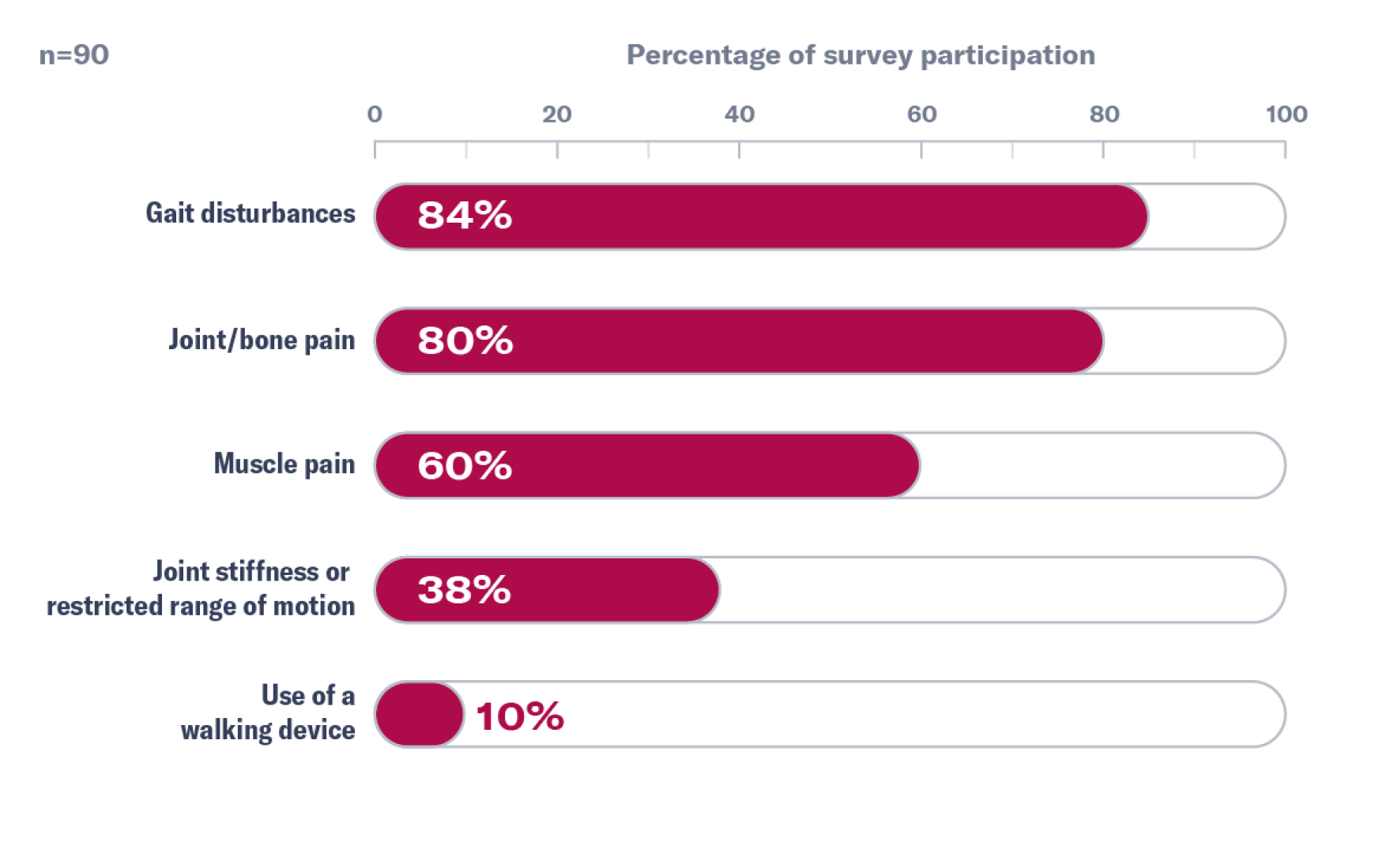
Most survey respondents reported a history of clinical symptoms that can impact mobility, such as gait disturbances, pain, and restrictions in range of motion.3

* These data are taken from a 2019 burden of disease study conducted in 90 pediatric patients with XLH. This component is from an international survey of parents and caregivers of children with XLH that reported below-normal health-related quality of life assessments.3
Children with XLH often present with short stature and lower extremity abnormalities, both of which may affect their mental health and self-esteem.3,7

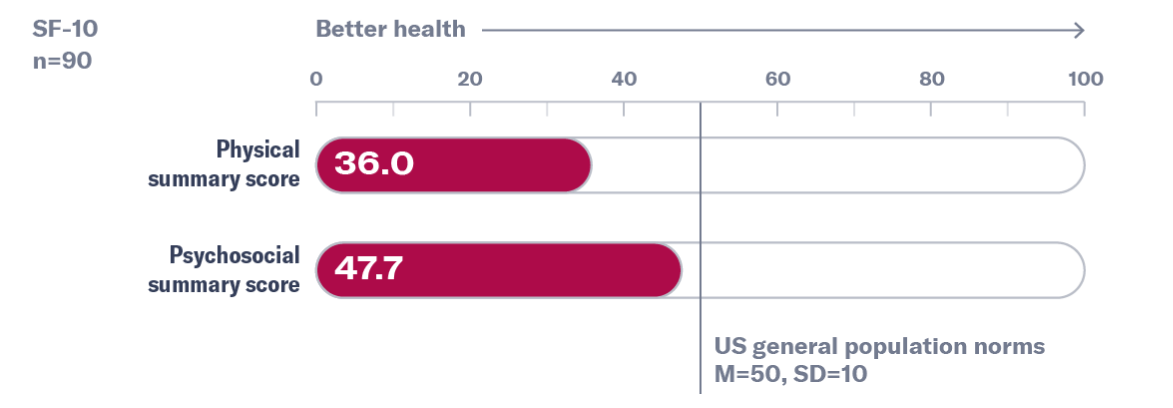
The SF-10 Health Survey for Children is a 10-question, parent-completed survey designed to measure health-related quality of life in children. The scoring method evaluated 2 summary measures: a physical summary score and a psychosocial summary score.8
*These data are taken from a 2019 burden-of-disease study conducted in 90 pediatric patients with XLH. This component is from an international survey of parents and caregivers of children with XLH that reported below-normal health-related quality of life assessments.3

Accurate diagnosis and early disease management can help minimize the lifelong XLH burden on your patients. Learn more about diagnosing XLH.
The burden of XLH starts in childhood and can worsen over time. Due to the progressive and chronic nature of XLH, adults may have unresolved XLH symptoms from childhood along with new symptoms. These unresolved symptoms can result in long-term consequences. XLH can manifest as chronic pain, frequent fractures, and physical mobility limitations for patients.3,9,10
Adults with XLH experienced more pain and stiffness compared with the general population.3

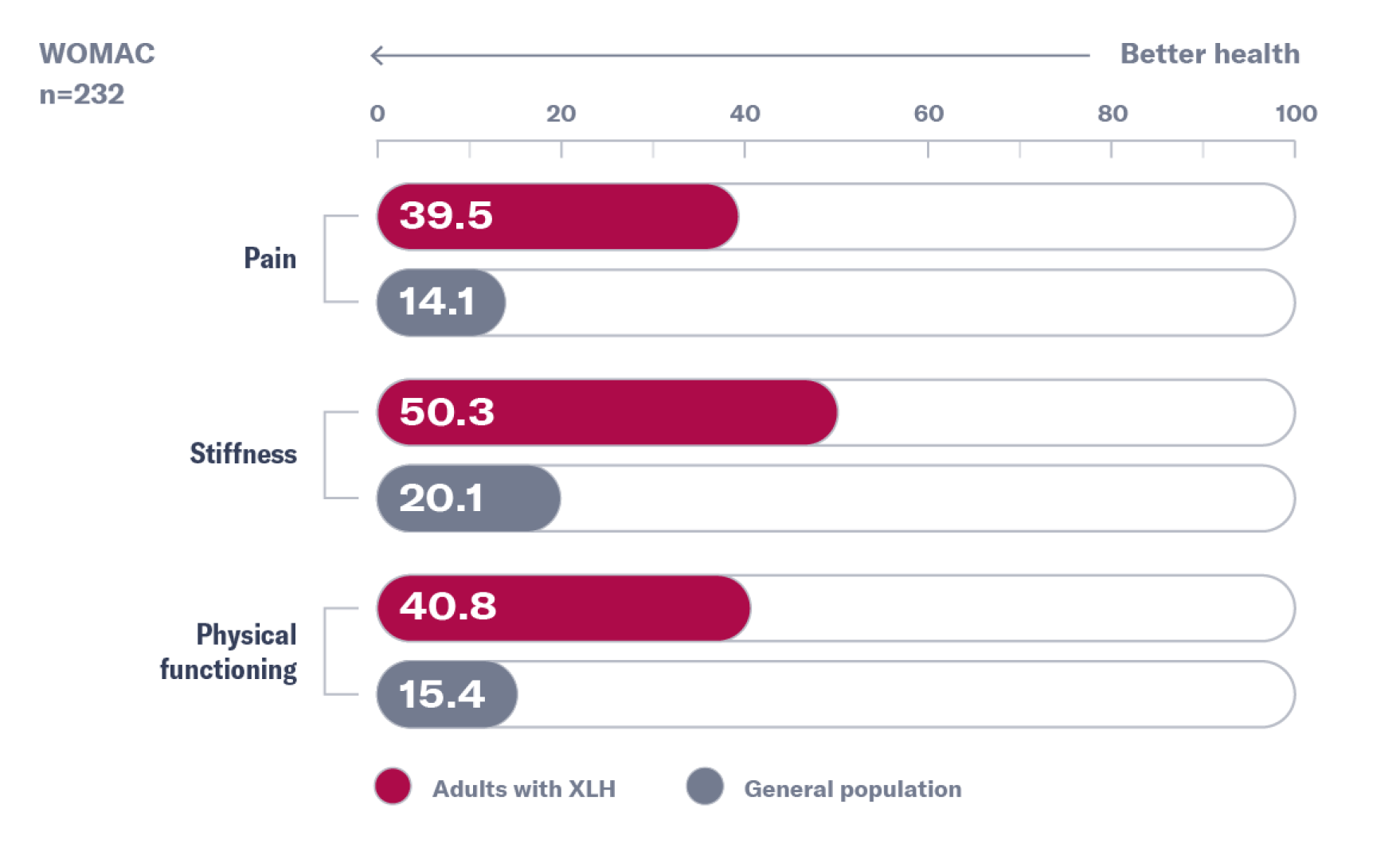
These data are taken from an international burden-of-disease study conducted in 232 adult patients with XLH.3
Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) is a questionnaire designed to assess pain, stiffness, and physical function in patients with hip and/or knee osteoarthritis. It has been used in patients with different conditions, including low back pain, rheumatoid arthritis, juvenile rheumatoid arthritis, systemic lupus erythematosus, and fibromyalgia.14
On average, approximately:
In a 2017 study consisting of 29 adults with XLH:
Many patients also suffer from pain, and some adults may require the use of a walking device.3
In a 2017 survey of 186 adults with XLH, 84% of adults believed that over time, their chronic hypophosphatemia had a greater impact and affected more areas of their lives.1
In a 2019 survey, the majority of patients reported negative social experiences as a result of their XLH, including bullying and unwanted social attention, that often resulted in low self-esteem, frustration, and depression.16
Adults with XLH may require long-term disease management to prevent further damage from chronic hypophosphatemia. Find out more about managing XLH.

Connect their symptoms and accurately diagnose with the right tests.

Learn more about how to accurately diagnose XLH through testing.

Manage XLH early to prevent progressive bone damage.
Set up time with a representative to talk more about XLH, or sign up for news and information about XLH.
References:
1. Hamilton AA, Faitos S, Jones G, Kinsley A, Gupta RN, Lewiecki EM. Whole body, whole life, whole family: patients' perspectives on X-linked hypophosphatemia. J Endocr Soc. 2022;6(8):bvac086. doi:10.1210/jendso/bvac086 2. Ruppe MD. X-linked hypophosphatemia. In: Adam MP, Everman DB, Mirzaa GM, et al., eds. GeneReviews®. Seattle (WA): University of Washington, Seattle; February 9, 2012. Updated April 13, 2017. https://www.ncbi.nlm.nih.gov/books/NBK83985/ 3. Skrinar A, Dvorak-Ewell M, Evins A, et al. The lifelong impact of X-linked hypophosphatemia: results from a burden of disease survey. J Endocr Soc. 2019;3(7):1321-1334. doi:10.1210/js.2018-00365 4. Mao M, Carpenter TO, Whyte MP, et al. Growth curves for children with X-linked hypophosphatemia. J Clin Endocrinol Metab. 2020;105(10):3243-3249. doi:10.1210/clinem/dgaa495 5. Centers for Disease Control and Prevention. Clinical growth charts. Children 2 to 20 years. Published May 30, 2000. Accessed May 21, 2019. https://www.cdc.gov/growthcharts/clinical_charts.htm. 6. Murali CN, Cuthbertson D, Slater B, et al. Pediatric outcomes data collection instrument is a useful patient-reported outcome measure for physical function in children with osteogenesis imperfecta. Genet Med. 2020;22(3):581-589. doi:10.1038/s41436-019-0688-6 7. Nguyen C, Celestin E, Chambolle D, et al. Oral health-related quality of life in patients with X-linked hypophosphatemia: a qualitative exploration. Endocr Connect.2022;11(1):e210564. doi:10.1530/EC-21-0564 8. Ramanuj PP, Granerød J, Davies NW, Conti S, Brown DW, Crowcroft NS. Quality of life and associated socio-clinical factors after encephalitis in children and adults in England: a population-based, prospective cohort study. PLoS One. 2014;9(7):e103496. doi:10.1371/journal.pone.0103496 9. Carpenter TO, Imel EA, Holm IA, Jan de Beur SM, Insogna KL. A clinician's guide to X-linked hypophosphatemia. J Bone Miner Res. 2011;26(7):1381-1388. doi:10.1002/jbmr.340 10. Linglart A, Biosse-Duplan M, Briot K, et al. Therapeutic management of hypophosphatemic rickets from infancy to adulthood. Endocr Connect. 2014;3(1):R13-R30. doi:10.1530/EC-13-0103 11. Steele A, Gonzalez R, Garbalosa JC, et al. Osteoarthritis, osteophytes, and enthesophytes affect biomechanical function in adults with X-linked hypophosphatemia. J Clin Endocrinol Metab. 2020;105(4):e1798-e1814. doi:10.1210/clinem/dgaa064 12. Skrinar A, Marshall A, San Martin J, Dvorak-Ewell M. X-linked hypophosphatemia (XLH) impairs skeletal health outcomes and physical function in affected adults. Poster presented at: The Endocrine Society Annual Meeting; March 5-8, 2015; San Diego, CA. 13. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Lawrence Erlbaum Associates; 1988. 14. Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). Rheumatology.org. Accessed March 7, 2018. 15. Yanes MIL, Diaz-Curiel M, Peris P, et al. Health-related quality of life of X-linked hypophosphatemia in Spain. Orphanet J Rare Dis. 2022;17(1):298. doi:10.1186/s13023-022-02452-0 16. Lo SH, Lachmann R, Williams A, Piglowska N, Lloyd AJ. Exploring the burden of X-linked hypophosphatemia: a European multi-country qualitative study. Qual Life Res. 2020;29(7):1883-1893. doi:10.1007/s11136-020-02465-x