Diagnosing XLH
Learn more about how to accurately diagnose XLH through testing.
XLH is the most common cause of inherited phosphorus wasting and leads to poor bone mineralization, resulting in rickets and osteomalacia.1,2,4,6

XLH can impact the skeletal, muscular, and dental health of children and adults throughout their lives and may require lifelong management.1,2,5,6
Increased FGF23 activity is the underlying cause of chronic hypophosphatemia1

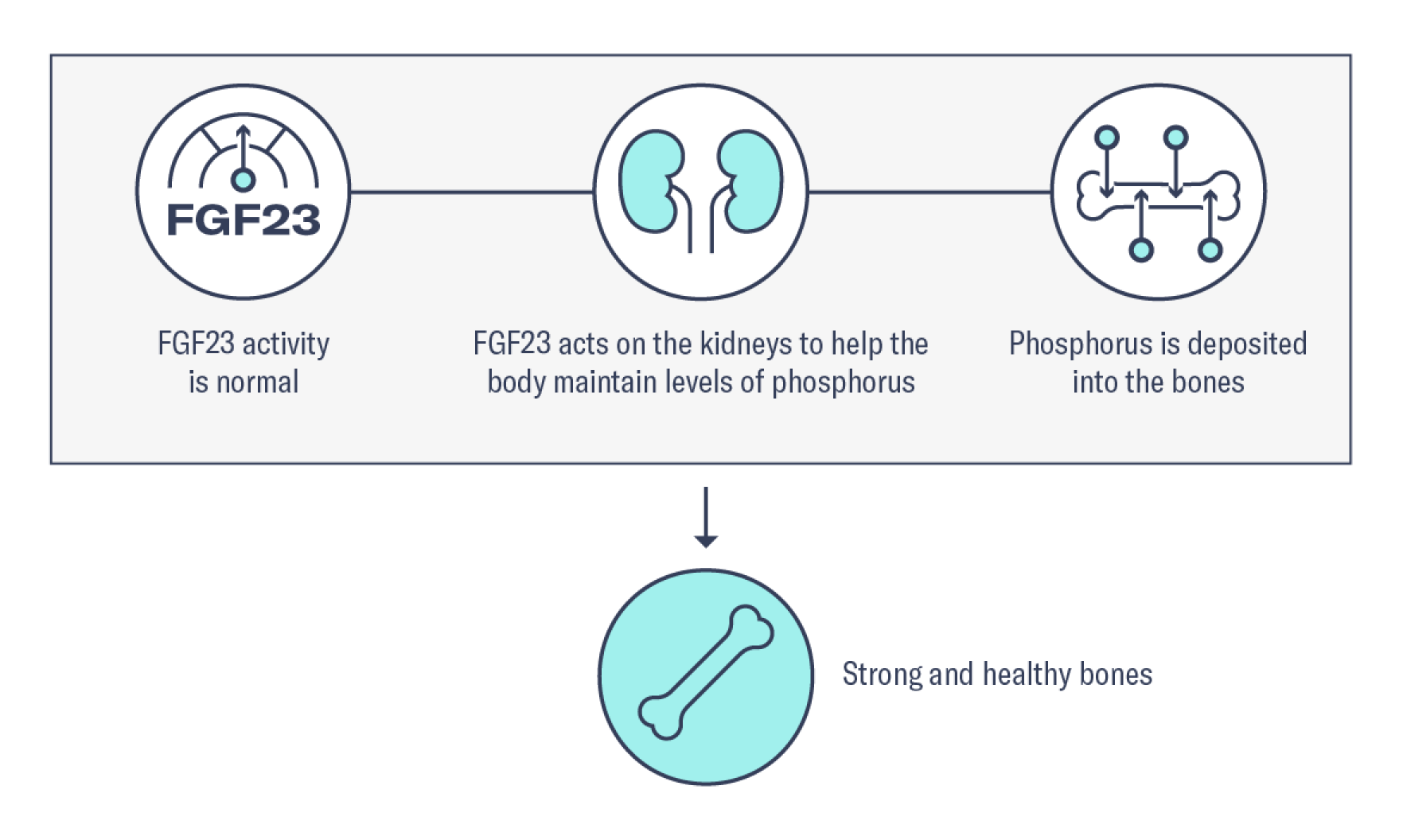
In normal homeostasis, FGF23 is a protein hormone produced by osteocytes in the bones that regulates serum phosphorus levels.12

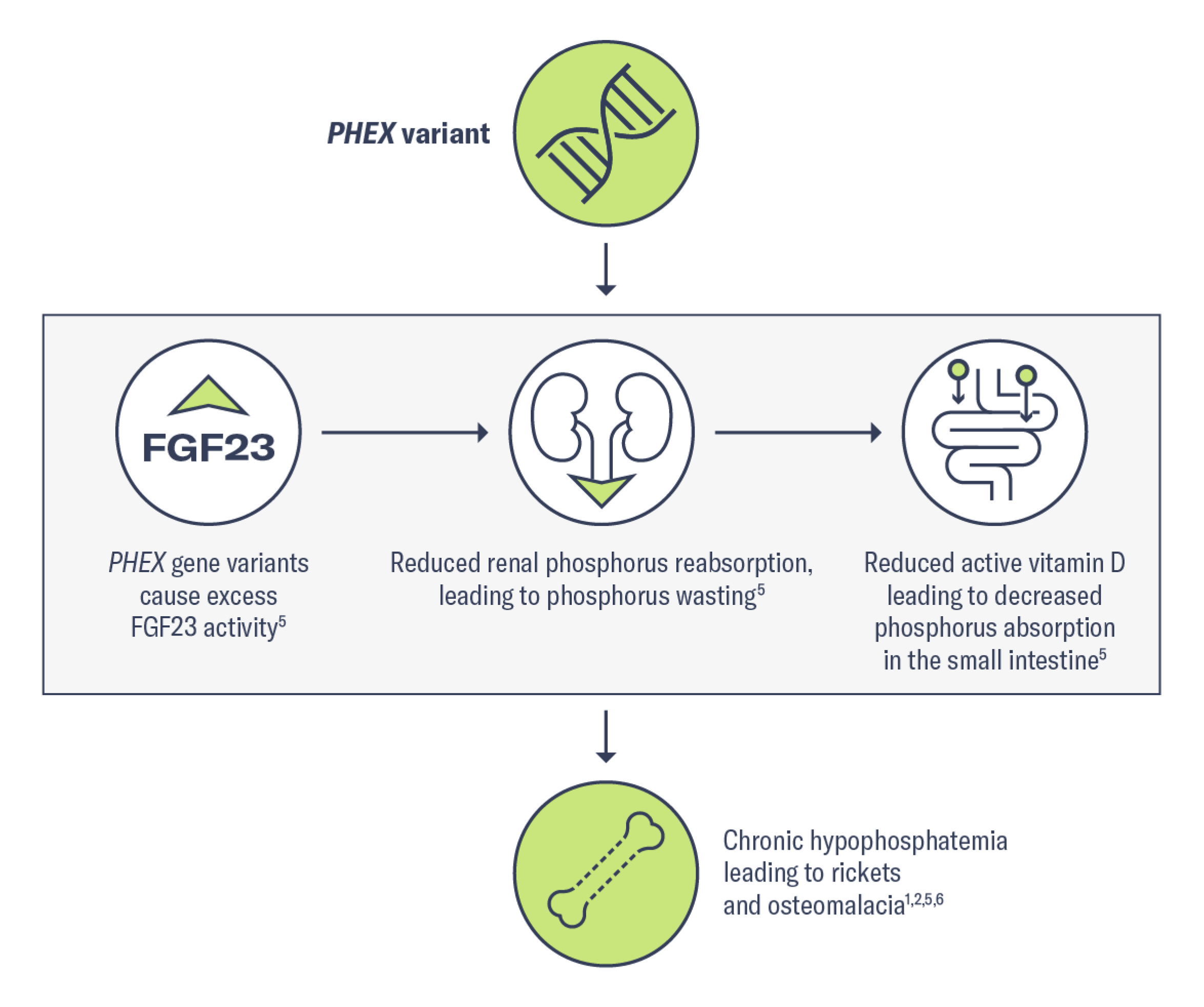
In XLH, a variant in the PHEX gene causes excess FGF23, which results in phosphorus wasting leading to chronic hypophosphatemia. Due to increased FGF23 activity, patients with XLH may experience skeletal defects, muscular dysfunction, and dental abnormalities.1,2,6
Gain a deeper understanding about the role of FGF23 in phosphorus regulation

XLH is often misdiagnosed as nutritional rickets or osteomalacia, hypophosphatasia, Pyle disease, or physiologic bowing.1
Misdiagnoses may lead to inappropriate disease management.13 Learn more about testing for XLH and how to get an accurate diagnosis for your patients.
Minimize the impact of XLH on your patients with an accurate diagnosis and early management of the disease.

Learn more about how to accurately diagnose XLH through testing.

Manage XLH early to prevent progressive bone damage.

From case studies to brochures, find resources for you and your patients to understand more about this rare condition.
Set up time with a representative to talk more about XLH, or sign up for news and information about XLH.
References:
1. Carpenter TO, Imel EA, Holm IA, Jan de Beur SM, Insogna KL. A clinician's guide to X-linked hypophosphatemia. J Bone Miner Res. 2011;26(7):1381-1388. doi:10.1002/jbmr.340 2. Ruppe MD. X-linked hypophosphatemia. In: Adam MP, Everman DB, Mirzaa GM, et al., eds. GeneReviews®. Seattle (WA): University of Washington, Seattle; February 9, 2012. Updated April 13, 2017. https://www.ncbi.nlm.nih.gov/books/NBK83985/ 3. Beck-Nielsen SS, Mughal Z, Haffner D, et al. FGF23 and its role in X-linked hypophosphatemia-related morbidity. Orphanet J Rare Dis. 2019;14(1):58. doi:10.1186/s13023-019-1014-8 4. Giannini S, Bianchi ML, Rendina D, Massoletti P, Lazzerini D, Brandi ML. Burden of disease and clinical targets in adult patients with X-linked hypophosphatemia. A comprehensive review. Osteoporos Int. 2021;32(10):1937-1949. doi:10.1007/s00198-021-05997-1 5. Dahir K, Roberts MS, Krolczyk S, Simmons JH. X-linked hypophosphatemia: a new era in management. J Endocr Soc. 2020;4(12):bvaa151. doi:10.1210/jendso/bvaa151 6. Linglart A, Biosse-Duplan M, Briot K, et al. Therapeutic management of hypophosphatemic rickets from infancy to adulthood. Endocr Connect. 2014;3(1):R13-R30. doi:10.1530/EC-13-0103 7. Fuente R, García-Bengoa M, Fernández-Iglesias Á, Gil-Peña H, Santos F, López JM. Cellular and molecular alterations underlying abnormal bone growth in X-linked hypophosphatemia. Int J Mol Sci. 2022;23(2):934. doi:10.3390/ijms23020934 8. X-linked hypophosphatemia. Genetic and Rare Diseases Information Center (GARD). Updated February 26, 2018. Accessed March 14, 2022. https://rarediseases.info.nih.gov/diseases/12943/x-linked-hypophosphatemia 9. Hereditary hypophosphatemic rickets. Genetics Home Reference. Updated August 18, 2020. Accessed March 14, 2022. https://ghr.nlm.nih.gov/condition/hereditary-hypophosphatemic-rickets 10. Wang M, Cao X, Cao B. Hypophosphatemic vitamin D-resistant osteomalacia: a case report. Exp Ther Med. 2013;6(3):791-795. doi:10.3892/etm.2013.1209 11. Aljuraibah F, Bacchetta J, Brandi ML, et al. An expert perspective on phosphate dysregulation with a focus on chronic hypophosphatemia. J Bone Miner Res. 2022;37(1):12-20. doi:10.1002/jbmr.4486 12. Martin A, Quarles LD. Evidence for FGF23 involvement in a bone-kidney axis regulating bone mineralization and systemic phosphate and vitamin D homeostasis. Adv Exp Med Biol. 2012;728:65-83. doi:10.1007/978-1-4614-0887-1_4 13. Trombetti A, Al-Daghri N, Brandi ML, et al. Interdisciplinary management of FGF23-related phosphate wasting syndromes: a Consensus Statement on the evaluation, diagnosis and care of patients with X-linked hypophosphataemia. Nat Rev Endocrino. 2022;18(6):366-384. doi:10.1038/s41574-022-00662-x